3 results
Integrated efficacy analysis from phase 3 studies of investigational microbiome therapeutic, SER-109, in recurrent Clostridioides difficile infection
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s5
-
- Article
-
- You have access
- Open access
- Export citation
-
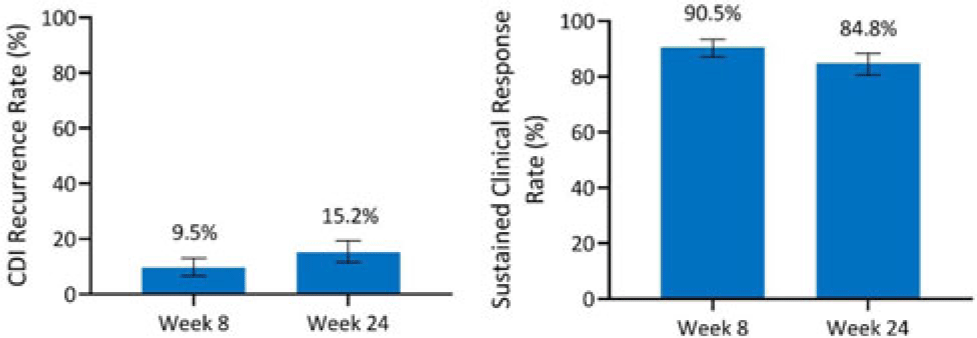
Background: Antibiotics alone are often insufficient to treat recurrent C. difficile infection (rCDI) because they have no activity against C. difficile spores that germinate within a disrupted microbiome. SER-109, an investigational, oral, microbiome therapeutic comprised of purified Firmicutes spores, was designed to reduce rCDI through microbiome repair. We report an integrated efficacy analysis through week 24 for SER-109 from phase 3 studies, ECOSPOR III and ECOSPOR IV. Methods: ECOSPOR III was a randomized, placebo-controlled phase 3 trial conducted at 56 US or Canadian sites that included 182 participants with ≥2 CDI recurrences, confirmed via toxin EIA testing. Participants were stratified by age (<65 years or ≥65 years) and antibiotic regimen (vancomycin, fidaxomicin) and were randomized 1:1 to placebo or SER-109 groups. ECOSPOR IV was an open-label, single-arm study conducted at 72 US or Canadian sites including 263 participants with rCDI enrolled in 2 cohorts: (1) rollover participants from ECOSPOR III who experienced on-study recurrence diagnosed by toxin EIA (n = 29) and (2) participants with ≥1 CDI recurrence (diagnosed by PCR or toxin EIA), inclusive of the current episode (n = 234). In both studies, the investigational product was administered orally as 4 capsules over 3 consecutive days following symptom resolution after standard-of-care antibiotics. The primary efficacy end point was rCDI (recurrent toxin-positive diarrhea requiring treatment) through week 8. Other end points included CDI recurrence rates and safety through 24 weeks. Results: These 349 participants received at least 1 dose of SER-109 in ECOSPOR III or ECOSPOR IV (mean age 64.2; 68.8% female). Overall, 77 participants (22.1%) enrolled with their first CDI recurrence. Four participants received blinded SER-109 in ECOSPOR III followed by a second dose of open-label SER-109 in ECOSPOR IV. Overall, the proportion of participants who received any dose of SER-109 with rCDI at week 8 was 9.5% (33 of 349; 95% CI, 6.6 %–13.0%), and the CDI recurrence rate remained low through 24 weeks (15.2%, 53 of 349; 95% CI, 11.6%–19.4%), corresponding to sustained clinical response rates of 90.5% (95% CI, 87.0%–93.4%) and 84.8% (95% CI, 80.6%–88.4%), respectively (Fig. 1). Most rollover participants (25 of 29, 86.2%) were from the placebo arm; 13.8% had rCDI by week 8. Conclusions: In this integrated analysis, the rates of rCDI were low and durable in participants who received the investigational microbiome therapeutic SER-109, with sustained clinical response rates of 90.5% and 84.8% at weeks 8 and 24, respectively. These data further support the potential benefit of microbiome repair with SER-109 following antibiotics for rCDI to prevent recurrence in high-risk patients.
Financial support: This study was funded by Seres Therapeutics.
Disclosure: None

Integrated safety analysis of phase 3 studies for investigational microbiome therapeutic, SER-109, in recurrent CDI
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s44-s45
-
- Article
-
- You have access
- Open access
- Export citation
Healthcare resource utilization in a phase 3 trial of SER-109 in patients with recurrent Clostridioides difficile infection
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s73
-
- Article
-
- You have access
- Open access
- Export citation
-
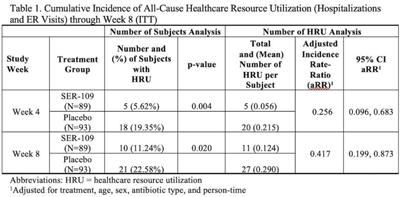
Background: The estimated economic cost of Clostridioides difficile infection (CDI) is $5.4 billion annually, primarily attributed to acute-care costs. We previously reported data from ECOSPOR III that SER-109, an investigational oral microbiome therapeutic, was superior to placebo in reducing recurrent CDI (rCDI) in adults at 8 weeks after treatment, with a 68% relative risk reduction. Adults with rCDI have more hospitalizations and emergency room (ER) visits (defined herein as healthcare resource utilization, HRU) compared to those without recurrence. Thus, we evaluated incidence of HRU. Methods: Adults with rCDI (≥3 episodes in 12 months) were screened at 56 US and Canadian sites and were randomized 1:1 to SER-109 (4 capsules × 3 days) or placebo following resolution of CDI with standard-of-care CDI antibiotics. The primary end point was rCDI at 8 weeks. Exploratory end points included cumulative incidence of hospitalizations through 24 weeks after treatment. Here, we report cumulative incidence of all-cause HRU through 8 weeks after treatment. Results: In total, 281 patients were screened and 182 were randomized (59.9% female; mean age 65.5 years; 98.9% outpatient). Overall, 31 patients (17%) had 38 hospitalizations or ER visits through week 8 (11 events in 10 SER-109 patients and 27 events in 21 placebo patients) (Table 1). The cumulative incidence of HRU was lower in SER-109–treated patients compared to placebo at both weeks 4 and 8 with most events (65.8%) recorded within 4 weeks after treatment. The adjusted HRU incidence rate (by person time, age, sex, and antibiotic use) was also lower in SER-109–treated patients compared to placebo at weeks 4 and 8 (0.256 [95% CI, 0.096–0.683] versus 0.417 [95% CI, 0.199–0.873], respectively). Conclusions: SER-109–treated patients had less HRU compared to placebo patients through 8 weeks after treatment in this mostly outpatient population. These data suggest a potential benefit of SER-109 in reducing HRU, thus lowering the healthcare burden of rCDI.
Funding: Seres Therapeutics
Disclosures: None